Tennis elbow / Lateral epicondylitis

DEFINITION
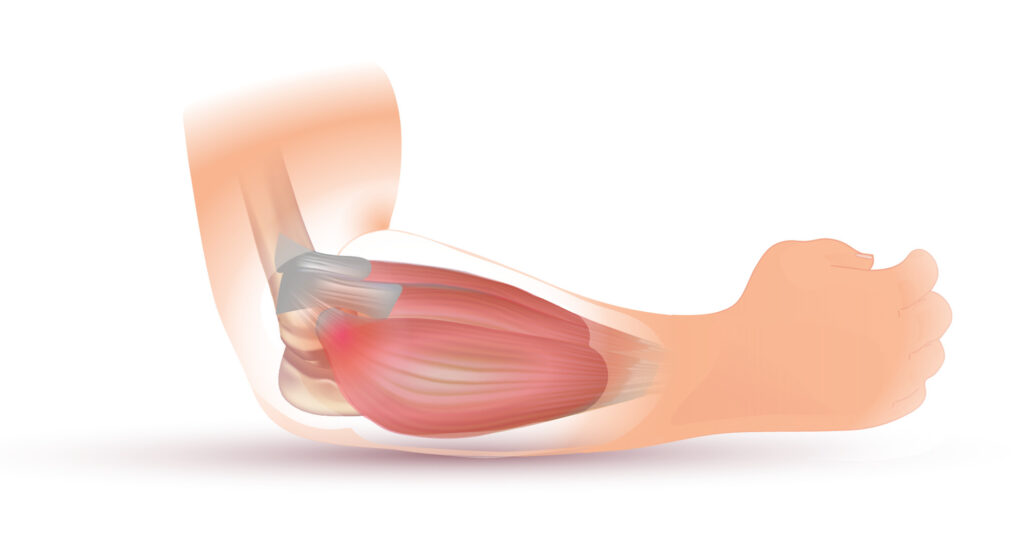
– Tennis elbow is commonly characterized by pain and tenderness at the origin of extensor group of muscle.
– It is usually due to overuse injury in day to day activities of pulling, lifting etc.
– Abnormal tissue has large number of nociceptive fibers , hence painful .
– With continued use, Tendinosis becomes microscopic partial tear.
• Pathophysiology
✓ Stage 1 : Acute inflammation but no angioblastic invasion.
✓ Stage 2 : Chronic inflammation with some angioblastic invasion.
✓ Stage 3 : Chronic inflammation with extreme angioblastic invasion.

• Causes
– Epicondylitis
– Calcified deposits
– Inflammation of adventitious bursa.
– Sports / computer usage.
– Repetitive overactivity of wrist extension against resistance.
• Clinical features
– More common in women , believed to be a degenerative disorder.
– Tenderness.
– Pain of neurological origin.
• On examination
– Extensor carpi radialis brevis should be checked for tightness.
– Positive Mill’s test
– ULTT may produce pain

• Diagnostic test
– Cozen’s test
AIM: To identify lateral and medical epicondylitis
PATIENT POSITION : Patient is sitting with elbow in 90 degree and supported, resist wrist extension, wrist radial deviation and forearm pronation with finger fully flexed simultaneously.
POSITIVE SIGN :Pain in lateral epicondyle .
– MILLS TEST
AIM : To identify lateral epicondylitis.
PATIENT POSITION : Therapist passively pronates the patient forearm then flex the elbow
PSITIVE SIGN : Pain over the lateral epicondyle of humerus
• Management
(1) Conservative management
– Rest and mild exercise with elbow strap.
– Injection of local anesthesia and steroid ( NSAID’s )
– Control of pain , electrotherapy modalities.
– Soft tissue therapy , manual therapy.
– Trigger points , stretching of extensor carpi radialis brevis.
– Muscle strengthening.
– Counterforce bracing , taping.
(2) Mill’s maneuver.
– Forceful extension of fully flexed and pronated forearm after injection.
(3) Surgical treatment
✓ Indication : Severe pain for 6 weeks, marked and localized tenderness.
✓ Methods : Percutaneous release of epicondylar muscles, Bosworth technique of the excision.
Physiotherapy management
• Preventive management
– For common origin of extensor group of muscles : Forceful repeated jerky movements can be given.
– Activities that should be avoided are wringing washed clothes, using wrench, tightening screw, even a vigorous hand shake .
– These activities can cause tennis elbow commonly in mechanical professions and sports.
– Repeated supination movement using heavy weights should also be avoided.
– Strengthening exercise to extensor carpi radialis longus and brevis as well as supinator should be encouraged .
• Prevention of further damage :
– During acute phase : Adequate care and resting the elbow joint with proper support should be done.
– Avoid movements like supination , wrist extension, radial deviation, and tight grips to prevent repetitive stretch and trauma to affected muscles.
– Avoiding hasty mobilization : Hasty mobilization will cause repetitive breakdown of scar tissue which prolongs the inflammatory reaction and leads to adhesion formation.
• Restoration
– Strain and tear of muscle : tenderness at musculotendinous junction of extensor carpi radialis brevis.
– Epicondylitis : Tenderness at lateral epicondyle. Granulation tissue formation and adhesion may be present.
-Bursitis : Development of bursa in subtendinous space.
– Articular involvement : Joint movements are painful.
• Pt management following surgery
(1) Reduce pain and inflammation.
(2) For Joints which are free from Immobilization : Limb elevation and active movements can be given.
(3) Slow relaxed full ROM passive movements ( elbow, forearm, wrist, ).
(4) Mobilization of shoulder and shoulder girdle is given to avoid adhesive capsulities.
(5) Begin with active assisted exercise and progress to self resistive technique.
Ultrasound ,TENS, can be used to reduce pain.
(6) Functional movements like supination , wrist extension and strong grip should be avoided.
(7) Progress gradually to PRE . By 5-6 weeks, painless elbow, forearm, wrist movements should be encouraged.